How To Heal Bunions
Overview
 A bunion is the enlargement of the joint at the base of the big toe. It occurs as a result of the misalignment of the bones of the big toe. This leads to stretching of the ligaments and tendons around the big toe joint and causes soft tissue over the joint to become inflamed and painful. There may be additional bone formation (exostosis) in the joint and the skin around the joint may become red and tender. Over time the cartilage in the joint can break down, leading to arthritis.
A bunion is the enlargement of the joint at the base of the big toe. It occurs as a result of the misalignment of the bones of the big toe. This leads to stretching of the ligaments and tendons around the big toe joint and causes soft tissue over the joint to become inflamed and painful. There may be additional bone formation (exostosis) in the joint and the skin around the joint may become red and tender. Over time the cartilage in the joint can break down, leading to arthritis.
Causes
Bunions are a common problem experienced mostly by women. The deformity can develop from an abnormality in foot function, or arthritis, but is more commonly caused by wearing improper fitting footwear. Tight, narrow dress shoes with a constrictive toe box (toe area) can cause the foot to begin to take the shape of the shoe, leading to the formation of a bunion. Women who have bunions normally wear dress shoes that are too small for their feet. Their toes are squeezed together in their shoes causing the first metatarsal bone to protrude on the side of the foot. It is important for men and women to realize that wearing dress shoes and boots, which are tapered in the toe area, can cause the bunion to worsen to the point where surgery is necessary.
Symptoms
It is unusual to have much bunion or hallux valgus pain when out of shoe wear or at rest. There are exceptions to this and in particular if symptoms have been ignored during the day and the bunion has become very painful during the day then some symptoms may be present at night. The pain from the region of the great toe at rest or at night is however more often a symptom of an arthritic big toe (hallux rigidus) rather than a straightforward bunion. To confuse matters these two conditions can sometimes coexist. Bunion or hallux valgus pain is most often present when walking in enclosed shoes. There may be little bunion pain in sandals or barefoot. It is unusual to have much bunion pain when not putting weight on the foot or at night. If there is bunion pain at rest or at night then there may also be arthritic change within the toe.
Diagnosis
A doctor can very often diagnose a bunion by looking at it. A foot x-ray can show an abnormal angle between the big toe and the foot. In some cases, arthritis may also be seen.
Non Surgical Treatment
Treatment options vary with the type and severity of each bunion, although identifying the deformity early in its development is important in avoiding surgery. The primary goal of most early treatment options is to relieve pressure on the bunion and halt the progression of the joint deformity. A podiatrist may recommend these treatments. Padding and Taping, Often the first step in a treatment plan, padding the bunion minimizes pain and allows the patient to continue a normal, active life. Taping helps keep the foot in a normal position, thus reducing stress and pain. Medication, Anti-inflammatory drugs and cortisone injections are often prescribed to ease the acute pain and inflammation caused by joint deformities. Physical Therapy, Often used to provide relief of the inflammation and bunion pain. Ultrasound therapy is a popular technique for treating bunions and their associated soft tissue involvement. Orthotics, Shoe inserts may be useful in controlling foot function and may reduce symptoms and prevent worsening of the deformity. 
Surgical Treatment
Surgery is the only way to correct a bunion. A bunion will usually get worse over time, so if it's left untreated it's likely to get bigger and become more painful. If your bunion is causing a significant amount of pain and affecting your quality of life, your GP may refer you to be assessed for bunion surgery. The aim of surgery is to relieve pain and improve the alignment of your big toe. Surgery isn't usually carried out for cosmetic reasons alone. Even after surgery, there may still be limits to the styles of shoe you can wear. Bunion surgery is often carried out as a day procedure, which means you won't have to stay in hospital overnight. The procedure will either be carried out under a local anaesthetic or a general anaesthetic.
Prevention
Bunions often become painful if they are allowed to progress. But not all bunions progress. Many bunion problems can be managed without surgery. In general, bunions that are not painful do not need surgical correction. For this reason, orthopaedic surgeons do not recommend "preventive" surgery for bunions that do not hurt; with proper preventive care, they may never become a problem.
The Causes And Treatment Of Over-Pronation
Overview
?Pes Planus? is the medical term for flat feet. It comes from Latin, Pes = foot and Planus = plain, level ground. Very few people suffer from this condition, as a true flat foot is very rare. Less than 5% of the population has flat feet. The majority of the Australian population, however, has fallen arches (an estimated 60-70% of the population) known in the medical profession as ?excess pronation? or over-pronation. Over-pronation means the foot and ankle tend to roll inwards and the arch collapses with weight-bearing. This is a quite a destructive position for the foot to function in and may cause a wide variety of foot, leg and lower back conditions.
Causes
Acquired "Flat Feet" this develops over a period of time rather than at birth (unlike Congenital "Flat Feet"). In children, many different factors may contribute to the development of this condition such as the type of shoes that a child wears, a child's sitting or sleeping positions or it may occur as some type of compensation for other abnormalities located further up the leg. Compensation may occur due to the rupture (tearing) of ligaments or tendons in the foot. One common reason for this condition is that the foot is compensating for a tight Achilles Tendon. If this tendon is tight it may cause the foot to point downward away from the body. This gives the body the perception that the affected leg is longer in length and the body attempts to compensate for the perceived additional length by flattening out the foot arch in an attempt to provide balance and stability.
Symptoms
It is important to note that pronation is not wrong or bad for you. In fact, our feet need to pronate and supinate to achieve proper gait. Pronation (rolling inwards) absorbs shock and supination (rolling outwards) propels our feet forward. It is our body?s natural shock-absorbing mechanism. The problem is over-pronation i.e. the pronation movement goes too deep and lasts for too long, which hinders the foot from recovering and supinating. With every step, excess pronation impedes your natural walking pattern, causing an imbalance in the body and consequent excessive wear and tear in joints, muscles and ligaments. Some common complaints associated with over-pronation include Heel Pain (Plantar Fasciitis) ,Ball of foot pain, Achilles Tendonitis, Shin splints, Knee Pain, Lower Back Pain.
Diagnosis
Look at the wear on your shoes and especially running trainers; if you overpronate it's likely the inside of your shoe will be worn down (or seem crushed if they're soft shoes) from the extra strain.
Non Surgical Treatment
Treatment with orthotics will provide the required arch support to effectively reduce excessive pronation and restore the foot and its posture to the right biomechanical position. It should be ensured that footwear has sufficient support, for example, shoes should have a firm heel counter to provide adequate control.
Surgical Treatment
The MBA implant is small titanium device that is inserted surgically into a small opening between the bones in the hind-mid foot: the talus (ankle bone) and the calcaneus (heel bone). The implant was developed to help restore the arch by acting as a mechanical block that prevents the foot from rolling-in (pronation). In the medical literature, the success rate for relief of pain is about 65-70%. Unfortunately, about 40% of people require surgical removal of the implant due to pain.
?Pes Planus? is the medical term for flat feet. It comes from Latin, Pes = foot and Planus = plain, level ground. Very few people suffer from this condition, as a true flat foot is very rare. Less than 5% of the population has flat feet. The majority of the Australian population, however, has fallen arches (an estimated 60-70% of the population) known in the medical profession as ?excess pronation? or over-pronation. Over-pronation means the foot and ankle tend to roll inwards and the arch collapses with weight-bearing. This is a quite a destructive position for the foot to function in and may cause a wide variety of foot, leg and lower back conditions.
Causes
Acquired "Flat Feet" this develops over a period of time rather than at birth (unlike Congenital "Flat Feet"). In children, many different factors may contribute to the development of this condition such as the type of shoes that a child wears, a child's sitting or sleeping positions or it may occur as some type of compensation for other abnormalities located further up the leg. Compensation may occur due to the rupture (tearing) of ligaments or tendons in the foot. One common reason for this condition is that the foot is compensating for a tight Achilles Tendon. If this tendon is tight it may cause the foot to point downward away from the body. This gives the body the perception that the affected leg is longer in length and the body attempts to compensate for the perceived additional length by flattening out the foot arch in an attempt to provide balance and stability.
Symptoms
It is important to note that pronation is not wrong or bad for you. In fact, our feet need to pronate and supinate to achieve proper gait. Pronation (rolling inwards) absorbs shock and supination (rolling outwards) propels our feet forward. It is our body?s natural shock-absorbing mechanism. The problem is over-pronation i.e. the pronation movement goes too deep and lasts for too long, which hinders the foot from recovering and supinating. With every step, excess pronation impedes your natural walking pattern, causing an imbalance in the body and consequent excessive wear and tear in joints, muscles and ligaments. Some common complaints associated with over-pronation include Heel Pain (Plantar Fasciitis) ,Ball of foot pain, Achilles Tendonitis, Shin splints, Knee Pain, Lower Back Pain.
Diagnosis
Look at the wear on your shoes and especially running trainers; if you overpronate it's likely the inside of your shoe will be worn down (or seem crushed if they're soft shoes) from the extra strain.
Non Surgical Treatment
Treatment with orthotics will provide the required arch support to effectively reduce excessive pronation and restore the foot and its posture to the right biomechanical position. It should be ensured that footwear has sufficient support, for example, shoes should have a firm heel counter to provide adequate control.
Surgical Treatment
The MBA implant is small titanium device that is inserted surgically into a small opening between the bones in the hind-mid foot: the talus (ankle bone) and the calcaneus (heel bone). The implant was developed to help restore the arch by acting as a mechanical block that prevents the foot from rolling-in (pronation). In the medical literature, the success rate for relief of pain is about 65-70%. Unfortunately, about 40% of people require surgical removal of the implant due to pain.
Tips On How To Treat Calcaneal Apophysitis?
Overview
Sever?s disease is also known as calcaneal apophysitis, which is a medical condition that causes heel pain In one or both feet. The disease is known to affect children between the ages of 8 and 14. Sever?s disease occurs when part of the child?s heel known as the growth plate (calcaneal epiphysis) is attached to the Achilles tendon. This area can suffer injury when the muscles and tendons of the growing foot do not keep pace with bone growth. Therefore, the constant pain which one experiences at the back of the heel will make the child unable to put any weight on the heel. The child is then forced to walk on their toes. Toe gait- develops in which the child must change the way they walk to avoid placing weight on the heel. This can lead to other problems as well in the future.
Causes
Sever disease is more common in children who do regular sports or exercise that puts pressure on the heels. Activities such as running and jumping can put stress on the tight muscles and tendons.
Symptoms
A few signs and symptoms point to Sever?s disease, which may affect one or both heels. These include Pain at the heel or around the Achilles tendon, Heel pain during physical exercise, especially activities that require running or jumping, Worsening of pain after exercise, A tender swelling or bulge on the heel that is sore to touch, Calf muscle stiffness first thing in the morning, Limping, A tendency to tiptoe.
Diagnosis
Sever disease is most often diagnosed clinically, and radiographic evaluation is believed to be unnecessary by many physicians, but if a diagnosis of calcaneal apophysitis is made without obtaining radiographs, a lesion requiring more aggressive treatment could be missed. Foot radiographs are usually normal and the radiologic identification of calcaneal apophysitis without the absence of clinical information was not reliable.
Non Surgical Treatment
Occasionally, an orthotic may need to be prescribed for temporary or long-term correction of their foot biomechanics (eg flat feet or high arches). During the acute phase of Sever's disease a small heel rise or shock-absorbing heel cup placed under the heel pad of your child's foot may help to ease the symptoms. Your podiatrist or physiotherapist can assess your child's arch and guide you in the best management of your child's condition. We recommend that your child should never go barefooted during the painful stages of Sever's disease.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Sever?s disease is also known as calcaneal apophysitis, which is a medical condition that causes heel pain In one or both feet. The disease is known to affect children between the ages of 8 and 14. Sever?s disease occurs when part of the child?s heel known as the growth plate (calcaneal epiphysis) is attached to the Achilles tendon. This area can suffer injury when the muscles and tendons of the growing foot do not keep pace with bone growth. Therefore, the constant pain which one experiences at the back of the heel will make the child unable to put any weight on the heel. The child is then forced to walk on their toes. Toe gait- develops in which the child must change the way they walk to avoid placing weight on the heel. This can lead to other problems as well in the future.
Causes
Sever disease is more common in children who do regular sports or exercise that puts pressure on the heels. Activities such as running and jumping can put stress on the tight muscles and tendons.
Symptoms
A few signs and symptoms point to Sever?s disease, which may affect one or both heels. These include Pain at the heel or around the Achilles tendon, Heel pain during physical exercise, especially activities that require running or jumping, Worsening of pain after exercise, A tender swelling or bulge on the heel that is sore to touch, Calf muscle stiffness first thing in the morning, Limping, A tendency to tiptoe.
Diagnosis
Sever disease is most often diagnosed clinically, and radiographic evaluation is believed to be unnecessary by many physicians, but if a diagnosis of calcaneal apophysitis is made without obtaining radiographs, a lesion requiring more aggressive treatment could be missed. Foot radiographs are usually normal and the radiologic identification of calcaneal apophysitis without the absence of clinical information was not reliable.
Non Surgical Treatment
Occasionally, an orthotic may need to be prescribed for temporary or long-term correction of their foot biomechanics (eg flat feet or high arches). During the acute phase of Sever's disease a small heel rise or shock-absorbing heel cup placed under the heel pad of your child's foot may help to ease the symptoms. Your podiatrist or physiotherapist can assess your child's arch and guide you in the best management of your child's condition. We recommend that your child should never go barefooted during the painful stages of Sever's disease.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
What Causes Adult Aquired Flat Foot ?
Overview
Adult acquired is a very serious condition that can lead to many secondary deformities, not only within the foot but also in the knees, hips and back. This presentation discusses a new scientifically proven procedure that may be able to help realign and fix this problem at its root. 
Causes
The cause of posterior tibial tendon insufficiency is not completely understood. The condition commonly does not start from one acute trauma but is a process of gradual degeneration of the soft tissues supporting the medial (inner) side of the foot. It is most often associated with a foot that started out somewhat flat or pronated (rolled inward). This type of foot places more stress on the medial soft tissue structures, which include the posterior tibial tendon and ligaments on the inner side of the foot. Children nearly fully grown can end up with flat feet, the majority of which are no problem. However, if the deformity is severe enough it can cause significant functional limitations at that age and later on if soft tissue failure occurs. Also, young adults with normally aligned feet can acutely injure their posterior tibial tendon from a trauma and not develop deformity. The degenerative condition in patients beyond their twenties is different from the acute injuries in young patients or adolescent deformities, where progression of deformity is likely to occur.
Symptoms
Patients often experience pain and/or deformity at the ankle or hindfoot. When the posterior tibial tendon does not work properly, a number of changes can occur to the foot and ankle. In the earlier stages, symptoms often include pain and tenderness along the posterior tibial tendon behind the inside of the ankle. As the tendon progressively fails, deformity of the foot and ankle may occur. This deformity can include progressive flattening of the arch, shifting of the heel so that it no longer is aligned underneath the rest of the leg, rotation and deformity of the forefoot, tightening of the heel cord, development of arthritis, and deformity of the ankle joint. At certain stages of this disorder, pain may shift from the inside to the outside aspect of the ankle as the heel shifts outward and structures are pinched laterally.
Diagnosis
Examination by your foot and ankle specialist can confirm the diagnosis for most patients. An ultrasound exam performed in the office setting can evaluate the status of the posterior tibial tendon, the tendon which is primarily responsible for supporting the arch structure of the foot.
Non surgical Treatment
The adult acquired flatfoot is best treated early. There is no recommended home treatment other than the general avoidance of prolonged weightbearing in non-supportive footwear until the patient can be seen in the office of the foot and ankle specialist. In Stage I, the inflammation and tendon injury will respond to rest, protected ambulation in a cast, as well as anti-inflammatory therapy. Follow-up treatment with custom-molded foot orthoses and properly designed athletic or orthopedic footwear are critical to maintain stability of the foot and ankle after initial symptoms have been calmed. Once the tendon has been stretched, the foot will become deformed and visibly rolled into a pronated position at the ankle. Non-surgical treatment has a significantly lower chance of success. Total immobilization in a cast or Camwalker may calm down symptoms and arrest progression of the deformity in a smaller percentage of patients. Usually, long-term use of a brace known as an ankle foot orthosis is required to stop progression of the deformity without surgery. A new ankle foot orthosis known as the Richie Brace, offered by PAL Health Systems, has proven to show significant success in treating Stage II posterior tibial dysfunction and the adult acquired flatfoot. This is a sport-style brace connected to a custom corrected foot orthotic device that fits well into most forms of lace-up footwear, including athletic shoes. The brace is light weight and far more cosmetically appealing than the traditional ankle foot orthosis previously prescribed. 
Surgical Treatment
Surgical correction is dependent on the severity of symptoms and the stage of deformity. The goals of surgery are to create a more functional and stable foot. There are multiple procedures available to the surgeon and it may take several to correct a flatfoot deformity. Usually surgical treatment begins with removal of inflammatory tissue and repair of the posterior tibial tendon. A tendon transfer is performed if the posterior tibial muscle is weak or the tendon is badly damaged. The most commonly used tendon is the flexor digitorum longus tendon. This tendon flexes or moves the lesser toes downward. The flexor digitorum longus tendon is utilized due to its close proximity to the posterior tibial tendon and because there are minimal side effects with its loss. The remainder of the tendon is sutured to the flexor hallucis longus tendon that flexes the big toe so that little function is loss.
Do I Suffer Adult Aquired Flat Foot (AAF)?
Overview
Have you noticed that the medial arch of your foot is becoming flatter when you walk? You may be developing adult acquired flat foot. This condition is typically caused by a problem with a tendon on the medial side of your foot called the Posterior Tibial Tendon that is not functioning well. You may experience pain in the inner side of your foot when you walk. The affected foot appears to roll outwards (the sole of the foot is trying to face outwards) when you walk. This is called over-pronation of the foot. The back of your heel may start to point outwards (heel valgus). Over time you may lose the ability to tip toe on that foot as the posterior tibial tendon stretches out and it may eventually tear.
Causes
Women are affected by Adult Acquired Flatfoot four times more frequently than men. Adult Flatfoot generally occurs in middle to older age people. Most people who acquire the condition already have flat feet. One arch begins to flatten more, then pain and swelling develop on the inside of the ankle. This condition generally affects only one foot. It is unclear why women are affected more often than men. But factors that may increase your risk of Adult Flatfoot include diabetes, hypertension, and obesity.
Symptoms
Your feet tire easily or become painful with prolonged standing. It's difficult to move your heel or midfoot around, or to stand on your toes. Your foot aches, particularly in the heel or arch area, with swelling along the inner side. Pain in your feet reduces your ability to participate in sports. You've been diagnosed with rheumatoid arthritis; about half of all people with rheumatoid arthritis will develop a progressive flatfoot deformity.
Diagnosis
Clinicians need to recognize the early stage of this syndrome which includes pain, swelling, tendonitis and disability. The musculoskeletal portion of the clinical exam can help determine the stage of the disease. It is important to palpate the posterior tibial tendon and test its muscle strength. This is tested by asking patient to plantarflex and invert the foot. Joint range of motion is should be assessed as well. Stiffness of the joints may indicate longstanding disease causing a rigid deformity. A weightbearing examination should be performed as well. A complete absence of the medial longitudinal arch is often seen. In later stages the head of the talus bone projects outward to the point of a large "lump" in the arch. Observing the patient's feet from behind shows a significant valgus rotation of the heel. From behind, the "too many toes" sign may be seen as well. This is when there is abducution of the forefoot in the transverse plane allowing the toes to be seen from behind. Dysfunction of the posterior tibial tendon can be assessed by asking the patient to stand on his/her toes on the affected foot. If they are unable to, this indicates the disease is in a more advanced stage with the tendon possibly completely ruptured.
Non surgical Treatment
Orthoses (insoles, functional orthoses, ankle supports, braces, ankle foot orthoses (AFOs)) - are usually custom-made to increase the functional stability of the foot and improve the mechanical properties of the tendon as well as reducing the actual degree of strain on the tendon. This reduces pain and inflammation. Physiotherapy - exercises and physiotherapy are often used to increase mobility, strengthen the tendon itself, stretch your Achilles tendon as well as reduce pain. Once the tendon has been stretched (stage one), the heel starts rolling outwards. Total immobilisation in a cast may help the symptoms to subside and prevent progression of the deformity in a smaller percentage of patients. Long-term use of orthoses may help stop progression of the deformity and reduce pain without surgery. Non-surgical treatment is unlikely to prevent progression to stage three and four but may be chosen by some patients who either are unsuitable for surgery or prefer not to have surgery.

Surgical Treatment
Many operations are available for the treatment of dysfunction of the posterior tibial tendon after a thorough program of non-operative treatment has failed. The type of operation that is selected is determined by the age, weight, and level of activity of the patient as well as the extent of the deformity. The clinical stages outlined previously are a useful guide to operative care (Table I). In general, the clinician should perform the least invasive procedure that will decrease pain and improve function. One should consider the effects of each procedure, particularly those of arthrodesis, on the function of the rest of the foot and ankle.
Have you noticed that the medial arch of your foot is becoming flatter when you walk? You may be developing adult acquired flat foot. This condition is typically caused by a problem with a tendon on the medial side of your foot called the Posterior Tibial Tendon that is not functioning well. You may experience pain in the inner side of your foot when you walk. The affected foot appears to roll outwards (the sole of the foot is trying to face outwards) when you walk. This is called over-pronation of the foot. The back of your heel may start to point outwards (heel valgus). Over time you may lose the ability to tip toe on that foot as the posterior tibial tendon stretches out and it may eventually tear.
Causes
Women are affected by Adult Acquired Flatfoot four times more frequently than men. Adult Flatfoot generally occurs in middle to older age people. Most people who acquire the condition already have flat feet. One arch begins to flatten more, then pain and swelling develop on the inside of the ankle. This condition generally affects only one foot. It is unclear why women are affected more often than men. But factors that may increase your risk of Adult Flatfoot include diabetes, hypertension, and obesity.
Symptoms
Your feet tire easily or become painful with prolonged standing. It's difficult to move your heel or midfoot around, or to stand on your toes. Your foot aches, particularly in the heel or arch area, with swelling along the inner side. Pain in your feet reduces your ability to participate in sports. You've been diagnosed with rheumatoid arthritis; about half of all people with rheumatoid arthritis will develop a progressive flatfoot deformity.
Diagnosis
Clinicians need to recognize the early stage of this syndrome which includes pain, swelling, tendonitis and disability. The musculoskeletal portion of the clinical exam can help determine the stage of the disease. It is important to palpate the posterior tibial tendon and test its muscle strength. This is tested by asking patient to plantarflex and invert the foot. Joint range of motion is should be assessed as well. Stiffness of the joints may indicate longstanding disease causing a rigid deformity. A weightbearing examination should be performed as well. A complete absence of the medial longitudinal arch is often seen. In later stages the head of the talus bone projects outward to the point of a large "lump" in the arch. Observing the patient's feet from behind shows a significant valgus rotation of the heel. From behind, the "too many toes" sign may be seen as well. This is when there is abducution of the forefoot in the transverse plane allowing the toes to be seen from behind. Dysfunction of the posterior tibial tendon can be assessed by asking the patient to stand on his/her toes on the affected foot. If they are unable to, this indicates the disease is in a more advanced stage with the tendon possibly completely ruptured.
Non surgical Treatment
Orthoses (insoles, functional orthoses, ankle supports, braces, ankle foot orthoses (AFOs)) - are usually custom-made to increase the functional stability of the foot and improve the mechanical properties of the tendon as well as reducing the actual degree of strain on the tendon. This reduces pain and inflammation. Physiotherapy - exercises and physiotherapy are often used to increase mobility, strengthen the tendon itself, stretch your Achilles tendon as well as reduce pain. Once the tendon has been stretched (stage one), the heel starts rolling outwards. Total immobilisation in a cast may help the symptoms to subside and prevent progression of the deformity in a smaller percentage of patients. Long-term use of orthoses may help stop progression of the deformity and reduce pain without surgery. Non-surgical treatment is unlikely to prevent progression to stage three and four but may be chosen by some patients who either are unsuitable for surgery or prefer not to have surgery.
Surgical Treatment
Many operations are available for the treatment of dysfunction of the posterior tibial tendon after a thorough program of non-operative treatment has failed. The type of operation that is selected is determined by the age, weight, and level of activity of the patient as well as the extent of the deformity. The clinical stages outlined previously are a useful guide to operative care (Table I). In general, the clinician should perform the least invasive procedure that will decrease pain and improve function. One should consider the effects of each procedure, particularly those of arthrodesis, on the function of the rest of the foot and ankle.
Achilles Tendonitis Suffering
Overview
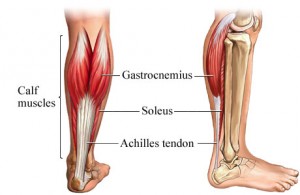
 Tendinitis is the inflammation of a tendon. Tendons are thick cords of tissue that connect muscles to bone. Achilles tendinitis, or an inflammation of the Achilles tendon, is one of the most common causes of foot or ankle pain. Other types of foot/ankle tendinitis include posterior tibial tendinitis and peroneal tendinitis.
Tendinitis is the inflammation of a tendon. Tendons are thick cords of tissue that connect muscles to bone. Achilles tendinitis, or an inflammation of the Achilles tendon, is one of the most common causes of foot or ankle pain. Other types of foot/ankle tendinitis include posterior tibial tendinitis and peroneal tendinitis.
Causes
Achilles tendinitis usually results from overuse and not a specific injury or trauma. When the body is subject to repetitive stress, the Achilles tendon is more prone to become inflamed. Other factors may cause Achilles tendinitis, such as, Sudden increase in physical activity, which can be related to distance, speed or hills, without giving yourself adequate time to adjust to the heightened activity. With running up hills, the Achilles tendon has to stretch more for each stride, which creates rapid fatigue. Inadequate footwear or training surface. High heels may cause a problem, because the Achilles tendon and calf muscles are shortened. While exercising in flat, athletic shoes, the tendon is then stretched beyond its normal range, putting abnormal strain on the tendon. Tight calf muscles which gives the foot a decreased range of motion. The strained calf muscles may also put extra strain on the Achilles tendon. Bone spur where the Achilles tendon attaches to the heel bone, aggravating the tendon and causing pain.
Symptoms
The onset of the symptoms of Achilles tendonitis tend to be gradual, with symptoms usually developing over a period of several days, or even weeks. Symptoms may include, Pain, this may be mild at first and may only be noticeable after exercise. Over time the pain may become constant and severe. Stiffness, this is usually relieved by activity. Sluggishness in the leg. Tenderness, particularly in the morning and most commonly felt just above where the tendon attaches to the heel bone. Swelling.
Diagnosis
Studies such as x-rays and MRIs are not usually needed to make the diagnosis of tendonitis. While they are not needed for diagnosis of tendonitis, x-rays may be performed to ensure there is no other problem, such as a fracture, that could be causing the symptoms of pain and swelling. X-rays may show evidence of swelling around the tendon. MRIs are also good tests identify swelling, and will show evidence of tendonitis. However, these tests are not usually needed to confirm the diagnosis; MRIs are usually only performed if there is a suspicion of another problem that could be causing the symptoms. Once the diagnosis of tendonitis is confirmed, the next step is to proceed with appropriate treatment. Treatment depends on the specific type of tendonitis. Once the specific diagnosis is confirmed, the appropriate treatment of tendonitis can be initiated.
Nonsurgical Treatment
Proper footwear with a strong and secure counter (the heel circumference) may help to encourage heeling of the tendon. A tendinitis will occasionally resolve on it?s own, with rest, ice, and gentle stretching. If symptoms persist for more than 2 weeks, consult your physician. Your physician may suggest physiotherapy and custom orthotics. Physiotherapy can suggest appropriate exercises and modalities to aid in the healing process. Custom orthotics can be very successful in treating the problem, as the original cause may be due to an improper alignment of the foot and heel. Re-aligning the foot to a neutral position may provide an optimal, biomechanically sound environment for healing to occur.
Surgical Treatment
Histological and biological studies on tendon healing have made it possible to envisage surgical repair using a percutaneous approach, with the following objectives, a minimal, and not very aggressive, operation, which is quick and easy and within the capabilities of all surgeons, the shortest hospitalisation period possible, above all, early and effective re-education, providing a satisfactory result both in terms of solidity and the comfort of the patient. The percutaneous tenosynthesis TENOLIG combines stability, reliability, patient comfort and lower overall social and professional costs for this type of lesion.
Prevention
A 2014 study looked at the effect of using foot orthotics on the Achilles tendon. The researchers found that running with foot orthotics resulted in a significant decrease in Achilles tendon load compared to running without orthotics. This study indicates that foot orthoses may act to reduce the incidence of chronic Achilles tendon pathologies in runners by reducing stress on the Achilles tendon1. Orthotics seem to reduce load on the Achilles tendon by reducing excessive pronation,
Tendinitis is the inflammation of a tendon. Tendons are thick cords of tissue that connect muscles to bone. Achilles tendinitis, or an inflammation of the Achilles tendon, is one of the most common causes of foot or ankle pain. Other types of foot/ankle tendinitis include posterior tibial tendinitis and peroneal tendinitis.
Causes
Achilles tendinitis usually results from overuse and not a specific injury or trauma. When the body is subject to repetitive stress, the Achilles tendon is more prone to become inflamed. Other factors may cause Achilles tendinitis, such as, Sudden increase in physical activity, which can be related to distance, speed or hills, without giving yourself adequate time to adjust to the heightened activity. With running up hills, the Achilles tendon has to stretch more for each stride, which creates rapid fatigue. Inadequate footwear or training surface. High heels may cause a problem, because the Achilles tendon and calf muscles are shortened. While exercising in flat, athletic shoes, the tendon is then stretched beyond its normal range, putting abnormal strain on the tendon. Tight calf muscles which gives the foot a decreased range of motion. The strained calf muscles may also put extra strain on the Achilles tendon. Bone spur where the Achilles tendon attaches to the heel bone, aggravating the tendon and causing pain.
Symptoms
The onset of the symptoms of Achilles tendonitis tend to be gradual, with symptoms usually developing over a period of several days, or even weeks. Symptoms may include, Pain, this may be mild at first and may only be noticeable after exercise. Over time the pain may become constant and severe. Stiffness, this is usually relieved by activity. Sluggishness in the leg. Tenderness, particularly in the morning and most commonly felt just above where the tendon attaches to the heel bone. Swelling.
Diagnosis
Studies such as x-rays and MRIs are not usually needed to make the diagnosis of tendonitis. While they are not needed for diagnosis of tendonitis, x-rays may be performed to ensure there is no other problem, such as a fracture, that could be causing the symptoms of pain and swelling. X-rays may show evidence of swelling around the tendon. MRIs are also good tests identify swelling, and will show evidence of tendonitis. However, these tests are not usually needed to confirm the diagnosis; MRIs are usually only performed if there is a suspicion of another problem that could be causing the symptoms. Once the diagnosis of tendonitis is confirmed, the next step is to proceed with appropriate treatment. Treatment depends on the specific type of tendonitis. Once the specific diagnosis is confirmed, the appropriate treatment of tendonitis can be initiated.
Nonsurgical Treatment
Proper footwear with a strong and secure counter (the heel circumference) may help to encourage heeling of the tendon. A tendinitis will occasionally resolve on it?s own, with rest, ice, and gentle stretching. If symptoms persist for more than 2 weeks, consult your physician. Your physician may suggest physiotherapy and custom orthotics. Physiotherapy can suggest appropriate exercises and modalities to aid in the healing process. Custom orthotics can be very successful in treating the problem, as the original cause may be due to an improper alignment of the foot and heel. Re-aligning the foot to a neutral position may provide an optimal, biomechanically sound environment for healing to occur.
Surgical Treatment
Histological and biological studies on tendon healing have made it possible to envisage surgical repair using a percutaneous approach, with the following objectives, a minimal, and not very aggressive, operation, which is quick and easy and within the capabilities of all surgeons, the shortest hospitalisation period possible, above all, early and effective re-education, providing a satisfactory result both in terms of solidity and the comfort of the patient. The percutaneous tenosynthesis TENOLIG combines stability, reliability, patient comfort and lower overall social and professional costs for this type of lesion.
Prevention
A 2014 study looked at the effect of using foot orthotics on the Achilles tendon. The researchers found that running with foot orthotics resulted in a significant decrease in Achilles tendon load compared to running without orthotics. This study indicates that foot orthoses may act to reduce the incidence of chronic Achilles tendon pathologies in runners by reducing stress on the Achilles tendon1. Orthotics seem to reduce load on the Achilles tendon by reducing excessive pronation,
What Is Painful Heel

Overview
The plantar fascia is a tough and flexible band of tissue that runs under the sole of the foot. It connects the heel bone with the bones of the foot, and acts as a kind of shock absorber to the foot. Sudden damage, or damage that occurs over many months or years, can cause tiny tears (microtears) to develop inside the tissue of the plantar fascia. This can cause the plantar fascia to thicken, resulting in heel pain. The surrounding tissue and the heel bone can also sometimes become inflamed.
Causes
Each time we take a step forward, all of our body weight first rests on the heel of one foot. As our weight moves forward, the entire foot begins to bear the body's weight, and the foot flattens and this places a great deal of pressure and strain on the plantar fascia. There is very little elasticity to the plantar fascia, so as it stretches only slightly; it pulls on its attachment to the heel. If the foot is properly aligned this pull causes no problems. However, if the foot is "pronated" (the foot rolls outward at the ankle, causing a break down of the inner side of the shoe), the arch falls excessively, and this causes an abnormal stretching of the relatively inflexible plantar fascia, which in turn pulls abnormally hard on the heel. The same pathology occurs with "supination" (the rolling inward of the foot, causing a break down of the outer side of the shoe). Supinated feet are relatively in flexible; usually have a high arch, and a short or tight plantar fascia. Thus as weight is transferred from the heel to the remainder of the foot, the tight plantar fascia hardly stretches at all, and pulls with great force on its attachment to the heel.
Symptoms
The symptoms of plantar fasciitis include pain in the bottom of your foot, especially at the front or centre of the heel bone, pain that is worse when first rising in the morning (called "first-step pain"), when first standing up after any long period of sitting, or after increased levels of activity especially in non-supportive shoes. Seek medical advice about plantar fasciitis if you have heel pain or pain in the bottom of your foot, especially when you get up in the morning, that does not respond to treatment or if there is redness or bruising in the heel.
Diagnosis
Your doctor can usually diagnose plantar fasciitis just by talking to you and examining your feet. Rarely, tests are needed if the diagnosis is uncertain or to rule out other possible causes of heel pain. These can include X-rays of the heel or an ultrasound scan of the fascia. An ultrasound scan usually shows thickening and swelling of the fascia in plantar fasciitis.
Non Surgical Treatment
About 80% of plantar fasciitis cases resolve spontaneously by 12 months; 5% of patients end up undergoing surgery for plantar fascia release because all conservative measures have failed. For athletes in particular, the slow resolution of plantar fasciitis can be a highly frustrating problem. These individuals should be cautioned not to expect overnight resolution, especially if they have more chronic pain or if they continue their activities. . Generally, the pain resolves with conservative treatment. Although no mortality is associated with this condition, significant morbidity may occur. Patients may experience progressive plantar pain, leading to limping (antalgic gait) and restriction of activities such as walking and running. In addition, changes in weight-bearing patterns resulting from the foot pain may lead to associated secondary injury to the hip and knee joints.

Surgical Treatment
The most dramatic therapy, used only in cases where pain is very severe, is surgery. The plantar fascia can be partially detached from the heel bone, but the arch of the foot is weakened and full function may be lost. Another surgery involves lengthening the calf muscle, a process called gastrocnemius recession. If you ignore the condition, you can develop chronic heel pain. This can change the way you walk and cause injury to your legs, knees, hips and back. Steroid injections and some other treatments can weaken the plantar fascia ligament and cause potential rupture of the ligament. Surgery carries the risks of bleeding, infection, and reactions to anesthesia. Plantar fascia detachment can also cause changes in your foot and nerve damage. Gastrocnemius resection can also cause nerve damage.